Introduction
Pain is among the most prevalent health conditions in the United States (U.S.), affecting approximately 50 million adults and representing one of the leading reasons individuals seek medical care.1 Clinical guidelines for musculoskeletal pain incorporate topical analgesics as first-line therapy as they help avoid risks of adverse effects from oral analgesics such as nonsteroidal anti-inflammatory drugs (NSAIDs) and opioids.2-4 Although select complementary therapies are recommended in pain treatment guidelines, homeopathy has not been included as an alternative option.3
Despite not being specifically recommended in conventional treatment guidelines, homeopathic medicines have been incorporated into practical pain management protocols.5 National survey data indicate that musculoskeletal conditions, especially pain, rank among the most frequently cited reasons for homeopathy use.6-8 According to a recent projection report, the homeopathy global market is expected to increase from $15.96 billion in 2025 to $28.81 billion by 2034, reflecting a 6.78% annual growth rate in the next decade.9
The increasing global use of homeopathic drug products (HDPs) offers an opportunity for pharmacy professionals to strengthen their understanding of homeopathy to enable them to meet rising demand for information and promote safe and appropriate use. Questions can arise in pharmacy practice regarding homeopathic products ranging from what homeopathy is to the safety of HDPs. This continuing education activity examines the role of homeopathy in pain management, with a focus on equipping pharmacy professionals with the knowledge needed to address common questions about homeopathic products and effectively counsel patients on their appropriate and safe use.
History of Homeopathy
Homeopathy was established by German physician Samuel Hahnemann, who grew disillusioned with 18th-century medicine and turned to translating scientific literature. While interpreting the work of Scottish physician William Cullen on Cinchona bark, which was a common malaria treatment at the time, Hahnemann was skeptical of Cullen’s explanation of how it worked. After ingesting a large dose of Cinchona himself, he developed malaria-like symptoms, including fever, chills, and fatigue. This finding led Hahnemann to hypothesize that a substance capable of producing certain symptoms in a healthy individual could cure those same symptoms in a sick patient, which became the foundational principle of homeopathy known as the Law of Similars, defined in Latin as similia similibus curentur, meaning “let like be cured by like.”10-11
Observing that standard doses often worsened symptoms before improvement, Hahnemann found that by reducing doses, this adverse effect was minimized without losing the therapeutic benefit, forming the second principle of homeopathy, the Law of Minimum Dose. Hahnemann further developed the potentization process of serial dilution combined with vigorous shaking, believing it helped to activate the healing properties of a substance.10
Together, the Law of Similars and the Law of Minimum Dose form the principles of homeopathy that state that a substance that causes symptoms in a healthy individual can, in extremely small doses, treat those same symptoms in someone who is ill.10
Overview of Homeopathy
Samuel Hahnemann coined the terms allopathy and homeopathy to describe two distinct treatment approaches: allopathy based on the principle of contraria contrariis, Latin for “opposites oppose,” and homeopathy, a philosophy based on the idea of “like cures like.” Today, allopathy refers to conventional medical treatments, while homeopathy is classified as a complementary therapy used as an adjunct to standard care.10
Homeopathy and Other Complementary Therapies
Complementary health approaches are broadly classified into two main categories: mind-body practices and natural products.12 Examples of mind-body practices include massages, meditation, acupuncture, tai chi, yoga, and others. Natural products primarily include dietary supplements such as herbal remedies, vitamins, minerals, amino acids, and probiotics. Homeopathic medicines are often confused with herbal remedies, yet the two are distinct types of complementary therapy.12 While both homeopathic medicines and dietary supplements are classified as natural products, homeopathic medicines are regulated as drugs, whereas dietary supplements are regulated as food.13
Homeopathic medicines and dietary supplements follow distinct federal regulatory standards, particularly in product labeling. Homeopathic labels must list active ingredients with potency dilutions, indications for use, and the “Homeopathic” designation, and may include limited therapeutic claims. In contrast, dietary supplements are restricted to structure and function claims only and cannot claim to diagnose, treat, cure, or prevent disease.13
Source Materials
Homeopathic medicines are prepared from plants, minerals, or animal-derived ingredients, with plant sources being the most common. Homeopathic products used for pain treatment include Arnica montana (mountain arnica or leopard’s bane), Rhus toxicodendron (poison oak or poison ivy), and Hypericum perforatum (St. John’s wort). Mineral and animal-derived extracts are also sources of several homeopathic products used in pain care. Examples of such pain-related products include Cuprum metallicum, which is derived from copper, and Apis mellifica, which is prepared from the honeybee.14-15
Manufacturing and Potentization
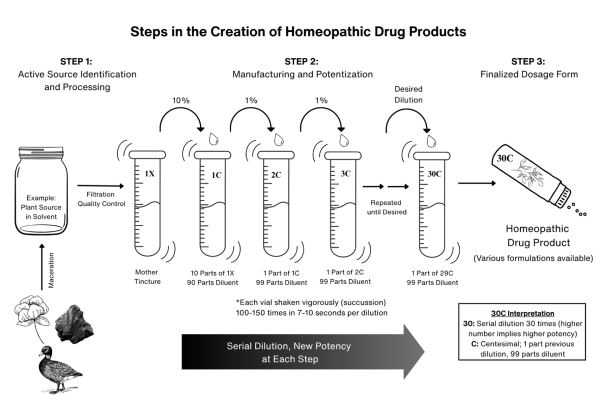
Homeopathic medicines are made through three main stages: raw material extraction and purification, potentization, and final product formulation.10,16 Homeopathic product manufacturing begins when the plant, mineral, or animal-derived ingredients are identified and processed under strict practice standards. Plant and animal-derived materials are macerated in water and alcohol solutions, while minerals are triturated or ground. The mixture is thereafter soaked to extract the active components, producing the base solution known as the mother tincture, which is stored under controlled conditions for further dilution.16
Potentization is a unique process in the creation of homeopathic products involving serial dilution and vigorous shaking, called succussion. This process uses standardized scales, most commonly the Centesimal (C) and Decimal (X) systems, which differ in their dilution ratios. Centesimal dilution follows a 1:100 ratio, where one part of the 1C preparation is diluted with 99 parts solvent to produce a 2C potency, followed by succussion. In contrast, the Decimal dilution uses a 1:10 ratio, diluting one part of a 1X preparation with nine parts of solvent to produce a 2X potency, also followed by succussion.10,16-17 Figure 1 illustrates the manufacturing and potentization process of a sample plant-based homeopathic medicine.
The final step involves preparing the dilutions into various formulations such as pellets, tablets, liquids, and topical creams, ointments, or gels. In the U.S. market, homeopathic products are commonly sold in Centesimal (6C, 30C) or Decimal (6X, 30X) potencies, mainly as over-the-counter (OTC) single medicines or multi-ingredient combinations packaged into branded products.10,18-19
Regulations of Homeopathic Drug Products
Under the Federal Food, Drug, and Cosmetic Act (FDCA) of 1938, homeopathic medicines are classified and regulated as drugs, primarily sold in the U.S. as OTC products. This classification places them under the regulatory authority of the Food and Drug Administration (FDA), requiring compliance with Good Manufacturing Practices (GMP) encompassing manufacturing, labeling, storage, and handling.20
The FDA recognizes the Homeopathic Pharmacopoeia of the United States (HPUS) as the official reference for approximately 1,300 homeopathic active ingredients. Unlike conventional medications, HDPs are exempt from FDA premarket approval and clinical trials demonstrating safety and efficacy. Instead, they gain acceptance through HPUS monograph inclusion, which requires toxicology and therapeutic use data reviewed by experts in medicine, biology, chemistry, botany, pharmacy, and others.21-22
The Federal Trade Commission (FTC) oversees HDP advertising, requiring claims to be truthful, non-misleading, and substantiated. Homeopathic drug product labels must include active ingredients with potency designations (e.g., 6C, 30C), the “HPUS” notation, warnings, directions, and inactive ingredients. Homeopathic labels must also carry the disclaimer: “Claims based on traditional homeopathic practice, not accepted medical evidence. Not FDA evaluated.” 23-24
Pain Classification and Management
Pain is classified according to either its duration or its underlying pathophysiology. By duration, pain is categorized as acute or chronic. Acute pain has a sudden onset and typically lasts from one to six months, whereas chronic pain persists for longer than six months. Based on the underlying pathophysiology, pain is classified into three types: nociceptive, neuropathic, and nociplastic.2
Nociceptive pain, the most common type, stems from the activation of sensory receptors that detect tissue damage as a result of injury, inflammation, heat or cold stimuli, and pressure or overexertion. Nociceptive pain is further classified into either somatic or visceral pain. Somatic pain occurs as a result of activated receptors located in the skin, connective tissues, muscle, joints, and bones, producing localized, sharp pain. Common examples of somatic pain include skin lacerations, inflammation, musculoskeletal injuries, arthritis, and bone fractures.2 Visceral pain develops when receptors in the internal organs are triggered leading to deep, diffuse, non-localized, cramping pain. Appendicitis, irritable bowel syndrome, menstrual cramps, and heartburn are some examples of visceral pain.2
Neuropathic pain results from central or peripheral nerve damage, presenting as shooting, prickling, burning, or tingling sensations. Common examples of neuropathic pain include diabetic neuropathy, trigeminal neuralgia, and postherpetic neuralgia.2
Nociplastic pain, the least understood of the three pain types, is characterized by persistent, generalized, diffused pain that is often associated with fatigue, insomnia, and cognitive impairment.2 In this type of pain, there is no definitive evidence of tissue injury or nerve damage associated with nociceptive or neuropathic pain, respectively. Some examples of nociplastic pain include fibromyalgia, chronic fatigue, and chronic headaches.2
Although pain is classified according to the primary affected receptors, some conditions involve a mix of pain types. Examples of mixed pain conditions include low back pain, cancer-related pain, and postsurgical pain.2
The American College of Physicians and American Academy of Family Physicians clinical guideline recommends topical NSAIDs as first-line treatment for acute pain from non-low back, musculoskeletal injury because they provide effective analgesia with fewer safety concerns.3 Oral NSAIDs and acetaminophen are considered second-line options, offering short-term benefit but posing risks such as gastrointestinal, renal, cardiovascular, and hepatic toxicity, especially at higher doses or in high-risk patients.3-4 Opioids are discouraged due to limited benefits and high risk of adverse effects and misuse.2 Due to adverse effects and drug interactions associated with conventional oral analgesics, patients may opt for nonpharmacologic therapies such as acupressure and transcutaneous electrical nerve stimulation.3
Homeopathy in Pain Care
Selection of Homeopathic Medicines
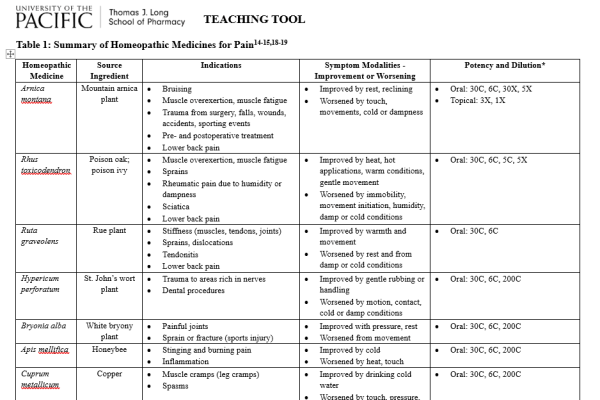
Common homeopathic medicines used as complementary therapies for pain include Arnica montana, Rhus toxicodendron, Ruta graveolens, Bryonia alba, and Hypericum perforatum.5,14-15 While these homeopathic medicines are indicated for pain, each product has specific characteristics that guide its individualized use.14-15
Arnica montana is derived from the perennial daisy plant commonly known as mountain arnica or leopard’s bane. Arnica is among the most widely used homeopathic medicines, commonly indicated for bruising, swelling from injury or acute trauma, muscle fatigue and soreness from overexertion, joint pain and stiffness, and perioperative pain.5,14-15 It is especially indicated for pain worsened by touch, physical movement, or exposure to cold, and is improved by rest or lying down.14-15 Low potencies of Arnica, primarily 1X and 3X, are available in single or combination topical preparations indicated for localized pain relief.14,18-19 Higher potencies, such as 6C and 30C, are formulated as oral or sublingual products and are generally considered when a broader range of symptoms is present.14,16,18
Rhus toxicodendron (Rhus tox) and Ruta graveolens are plant-based homeopathic medicines frequently used for symptoms of aching, bruising, stiffness, and numbness.5,14-15 These symptoms are typically worsened by initial movement, prolonged rest, and exposure to cold or damp environments, but relieved by slow movement and warmth.14-15Rhus tox, prepared from poison ivy or poison oak, is indicated for pain related to joint disorders (e.g. arthritis), injury or trauma, and muscular overexertion, and is especially useful for sprains, strains, and pain following dislocations or bone realignment.5,14-15 Ruta, derived from the rue plant native to southern Europe, is indicated for deep, aching pain from overexertion or injury to connective tissues, making it well-suited for conditions affecting tendons, ligaments, and periosteum, such as tendonitis, periostitis, and post-orthopedic trauma pain.5,14-15
Bryonia alba, sourced from the white bryony root, is indicated for sharp, localized pain that is aggravated by the slightest movement and is relieved with rest or firm pressure. It acts primarily on mucous and serous membranes and is particularly good for bursitis and pleuritis.5,14-15 Bryonia is frequently used in inflammatory conditions involving joints, pleuritic chest pain, and headaches that intensify with motion.14-15
Hypericum perforatum, derived from St. John’s wort, is mainly used for nerve-related pain that is characterized by sharp, shooting, or radiating sensations.5,14-15 Hypericum is particularly indicated for pain from injuries involving areas with rich nerve endings, such as the fingers, toes, or spine. It is especially useful for symptoms that are worsened by cold or damp environments and touch or sudden movement. Sometimes referred to as the “Arnica of the nerves,” Hypericum is indicated for nerve pain following tooth extractions, puncture wounds, surgical procedures, and phantom limb sensations.14-15
Table 1 lists commonly used homeopathic medicines as complementary therapies in the management of pain.14-15,18-19
Individualized vs. Non-Individualized Homeopathic Medicine
Homeopathic treatment selection is guided by distinct approaches of either individualized homeopathic medicine (IHM) or non-individualized homeopathic medicine (non-IHM). Individualized homeopathic medicine emphasizes the whole person’s “symptom totality” focusing on the primary complaint, in addition to the contributing or underlying causes, the quality and location of the sensations, factors that worsen or relieve the symptoms, and any associated physical or emotional conditions. Often, a single homeopathic medicine is selected based on the tailored approach of IHM.10-11
In contrast, non-IHM targets the specific disease pathology using one or more medicines to manage the different clinical symptoms.10 In non-IHM, multiple homeopathic medicines are often manufactured into a single product to treat common conditions such as colds, sleeplessness, and allergies.10-11 While potency is considered when choosing treatment, accurate selection of the appropriate homeopathic medicine is regarded as the most important factor in achieving therapeutic benefits.17
Homeopathy in Pain-Related Clinical Trials
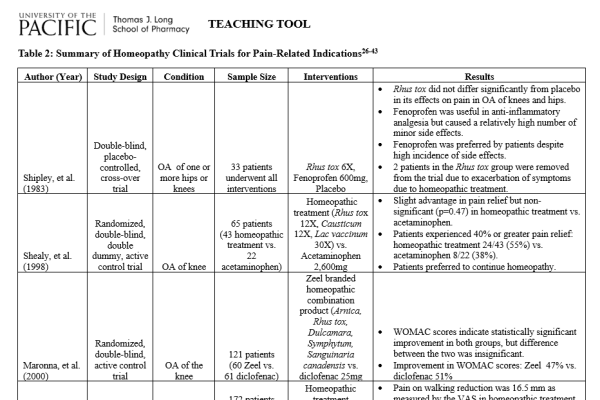
Health care professionals may encounter questions from patients regarding clinical evidence supporting the use of homeopathy for specific pain conditions. Randomized, controlled clinical trials have investigated homeopathic medicines as treatments for arthritis, musculoskeletal overexertion, and perioperative pain.25-43 Table 2 summarizes a sample of these clinical studies that have evaluated different homeopathic regimens, including non-IHM, for pain-related indications.26-43
Arthritis
Arthritis is the inflammation of one or more joints resulting in pain, stiffness, swelling, reduced mobility, and impaired range of motion.44 Conventional arthritis treatment combines nonpharmacological measures with pharmacological therapies. Common nonprescription pain medications include acetaminophen, oral NSAIDs (e.g. ibuprofen, naproxen), and topicals such as diclofenac and trolamine that aim to reduce pain and improve daily function.45 However, their chronic use may be limited by adverse effects.4
Arnica montana topical preparations, homeopathic combination products, and IHM treatment approaches have been evaluated as potential treatments for arthritis. Investigators have evaluated their effectiveness, safety, and limitations in reducing arthritis-related pain.25-32
Koley et al. (2013) conducted a systematic review of clinical trials, published between 1980 and 2013, which evaluated the effectiveness of homeopathic treatments for osteoarthritis (OA).25 Eight trials including 1,444 patients examined homeopathic combination products rather than individualized homeopathy. Seven of the eight trials reported positive or non-inferior results in pain symptoms and function improvement comparable to standard NSAIDs and acetaminophen treatments. One study reported homeopathy was inferior to conventional NSAIDs and similar to placebo. Overall, the review suggests potential benefits of homeopathic combination products in OA but emphasizes the need for more well-designed trials, especially using individualized approaches.25
In a randomized, double-blind controlled trial by Widrig et al. (2007), 204 patients with hand OA were assigned to either topical Arnica gel (n=105) or topical ibuprofen gel (n=99); both treatments were applied to affected joints three times daily for three weeks. Both groups showed similar improvements in pain scores and hand functional ability. Both topical treatment groups were well tolerated, with no significant adverse effects (4.8% for topical Arnica compared to 6.1% for topical ibuprofen). However, the lack of a placebo control arm was a limitation to the study’s reported efficacy outcomes. Results suggest that topical Arnica was at least as effective as topical ibuprofen and may be a suitable alternative for patients with OA symptoms.30
Bhattacharyya et al. (2024) conducted a randomized, double-blind, placebo-controlled feasibility trial to evaluate the effects of IHMs in patients with knee OA. Forty participants were assigned to receive either IHM or placebo for two months as adjunctive therapy to standardized care. Compared to placebo, the IHM group showed statistically significant improvements across the Knee Injury and Osteoarthritis Outcome Score (KOOS) subscales, including stiffness symptoms (p < 0.001), pain (p = 0.002), activities of daily living (p < 0.001), sports/recreation (p = 0.016), and quality of life (p = 0.002). Most frequently used homeopathic medicines were Arnica, Sulphur, and Natrum muriaticum. No serious adverse events were reported. These findings suggest that IHMs may improve outcomes in knee OA, though larger trials are needed to confirm efficacy.32
Although early research failed to show that homeopathy outperformed placebo in OA management, more recent evidence suggests that certain IHMs may provide modest symptomatic relief when used as adjunctive OA therapy to standard care, although well-designed clinical trials are needed to confirm these results.26,30-32
Musculoskeletal Overexertion and Trauma
Musculoskeletal pain occurs when muscles, tendons, and joints are overworked, stressed beyond their normal capacity, or damaged from injury. Patients who experience musculoskeletal overexertion or trauma present with localized muscle soreness, worsened by movement or touch, and possible inflammation.46 Several studies have sought to examine the effects of Arnica montana in post-exercise recovery and muscle soreness.33-35
Tveiten and Bruset (2003) reported on two randomized, double-blind, placebo-controlled trials of 82 marathon runners who received either Arnica montana (n=44) or placebo (n=38) following a race. Muscle soreness was measured by visual analogue scale (VAS) scores, and cell damage was measured by muscle enzyme concentrations before, 42 hours, and 66 hours after the marathon. The Arnica group reported significantly less muscle soreness as measured by VAS scores the next day compared to the placebo group (p = 0.04). However, there were no significant differences in the muscle enzyme concentrations between the two groups. No adverse effects were reported. The findings indicate that Arnica montana may provide short-term relief from muscle soreness after intense exercise.34
In 2022, Bartolomei et al. reported the effects of a mud pack containing menthol and Arnica montana on recovery after a high-volume lower-body resistance training session in 10 participants, with five assigned to the mud pack group and five to the placebo group. The study found that the mud pack significantly reduced muscle soreness at 24 hours (p=0.002) and 48 hours (p=0.015) after exercise when compared to placebo. However, there were no significant differences in muscle performance measures or swelling. These findings suggest that the application of menthol and Arnica montana in the mud pack may help to alleviate muscle discomfort and expedite recovery following strenuous exercise but found no changes in muscle thickness. No serious adverse effects were reported. The authors emphasized the potential of such treatments in reducing the perception of muscle soreness.35
Vickers et al. (1998) randomized 400 patients to receive either Arnica montana 30X (n=200) or placebo (n=200) to examine their impact on muscle soreness after long-distance running. There was no difference in the VAS scores to measure 2-day and 5-day soreness. Adverse reactions were reported in 21 patients (9 and 12 in the Arnica and placebo groups, respectively).33
Although Vickers and colleagues reported that Arnica montana 30X was not effective in reducing muscle soreness, other studies involving non-IHM Arnica formulations have suggested that Arnica may help alleviate soreness and promote recovery following exercise-induced strain or minor injury.33-35 Nevertheless, further research is needed to confirm these findings, particularly studies focusing on IHM-based treatments.
Perioperative Pain
Perioperative pain occurs before, during, and after surgery from causes such as incisions and inflammation. Practice guidelines recommend multimodal treatment by combining pain medications such as nonprescription analgesics and opioids with nonpharmacologic measures. While this approach is effective for pain management, oral analgesics have adverse effects.4, 47-48
Studies have investigated the potential role of homeopathy to reduce pain, minimize conventional drug consumption, and enhance outcomes in perioperative pain management.36-43
In a meta-analysis, Gaertner et al. evaluated whether Arnica montana improves postoperative recovery by reducing pain, bruising, swelling, and related complications. The analysis screened 23 publications yielding 28 comparisons of Arnica with placebo or active treatments in patients who underwent dental, facial, orthopedic, or hand surgeries and used different potencies and dosing schedules. Eighteen placebo-controlled comparisons formed the primary analysis. Outcome measures varied across trials, so each study’s results were converted into a standardized effect size (Hedge’s g).36
Across placebo-controlled trials, Arnica showed a small positive effect (g=0.18), narrowly missing statistical significance due to considerable heterogeneity (p=0.059). In studies where homeopathy was compared with active control (mostly NSAIDs), a modest effect favoring Arnica was reported but was driven by non-randomized studies; however, in randomized comparisons, Arnica and standard NSAIDs performed similarly. Trial heterogeneity reflects differences in surgical procedures, outcome measures, potencies, and study design. The authors concluded that homeopathic Arnica montana showed a small overall benefit for postoperative recovery with results trending toward a positive effect but did not achieve statistical significance.36
Robertson et al. (2007) conducted a randomized, double-blind, placebo-controlled trial of 190 adults undergoing tonsillectomy. Patients were randomized to receive either Arnica 30C (n=95) or placebo (n=95), with 111 participants completing questionnaires to report change in VAS pain scores over 14 days following the procedure. The Arnica group had significantly greater reduction in pain scores from day 1 to day 14 compared to placebo (p<0.05). No significant differences were observed for secondary outcomes of analgesic use, hospital visits, antibiotic consumption, day on which swallowing returned to normal, and day returned to work.40
Akay and Sanal (2024) conducted a three-arm controlled clinical trial to evaluate postoperative outcomes of oral standard therapy (antibiotic and NSAID), oral standard therapy plus topical Arnica, or oral standard therapy plus topical mucopolysaccharide polysulfate (MPSP) following mandibular molar surgery. Outcomes included pain as measured by VAS scores, trismus, and edema over a 10-day postoperative period. Pain intensity was lower in both adjunct treatment groups compared with standard therapy alone. Maximum mouth opening measurements indicated that Arnica significantly reduced trismus, while facial edema measurements showed that MPSP significantly decreased postoperative swelling. The authors concluded that both Arnica and MPSP may be beneficial complementary therapies in postoperative recovery following molar surgery.43
Product Safety
A systematic review of 41 observational studies found adverse effects associated with homeopathic medicines were minor to moderate in severity, comparable to those observed in control groups, and less frequent than those reported with conventional medicines or other complementary therapies.49
In 2017, the FDA introduced risk-based enforcement priorities for HDPs, emphasizing products with safety concerns, non-oral or topical preparations, vulnerable populations, quality deficiencies, or those claiming to treat serious conditions. This regulatory framework was finalized in 2022.50 While oral HDPs are highly diluted and must comply with GMP standards, topical preparations used in pain care often contain relatively higher concentrations of active ingredients. Although uncommon, some isolated adverse event cases have been reported.50 Health practitioners, patients, and consumers can report adverse events related to homeopathic medicines through the FDA’s MedWatch safety reporting program.51
Patient Care and Education
Homeopathic products are marketed as nonprescription drugs, positioning pharmacy professionals as an accessible source of information for patients and consumers. However, surveys show that many pharmacy practitioners have limited knowledge about homeopathy, despite homeopathy’s widespread availability.52 Pharmacy faculty in the U.S. emphasize the need for pharmacists to understand homeopathic products and to be capable of communicating effectively with patients.53
Pharmacists have clinical training in assessing self-limiting pain conditions and determining when self-care is suitable or if referral for further medical evaluation is warranted. When patients choose complementary therapies, pharmacists should advise when homeopathy may be suitable and when it is not. Patients should be informed that homeopathic medicines may be used as complementary therapies for certain self-limiting conditions, including pain, if desired, but they are not FDA-approved to treat or cure disease.
Patients should be advised to never delay or replace necessary medical care with homeopathic treatments. Education should include guidance to discontinue use or consult a health care provider if symptoms worsen, allergic reactions occur, or the condition fails to improve. Patients with known allergies to a homeopathic product’s source ingredient should avoid using it. Consumers should disclose all homeopathic products to their health care providers so that potential drug interactions can be assessed.
Consumers should verify that such products are labeled “Homeopathic’ and bearing the “HPUS” designation as the indicator for quality and standardization. Oral pellets should be dissolved sublingually, while topical preparations are for external use only, avoiding open wounds, eyes, and mouth.
The internet offers widespread access to homeopathy information. A national survey showed that more than half of adult Americans search for health information online, including through social media and mobile health apps.54 In addition to accredited educational materials, pharmacy professionals can utilize reputable online resources to help patients and consumers with point of care homeopathic product selection, if desired, and consultations regarding its proper use.
Homeopathic organizations supply online educational resources, including virtual webinars and digital materials, to inform both the public and health practitioners about homeopathy. The National Center for Homeopathy’s website features a “Find a Remedy” tool that helps users identify appropriate homeopathic options for various self-limiting conditions, including those affecting pets.55 Manufacturers’ websites and mobile apps are also available to assist consumers in finding homeopathic products for their self-limiting conditions, if desired.56 Additionally, pharmacy professionals can develop a general understanding of homeopathy, as well as targeted topics such as its use in oncologic palliative care, through accredited pharmacy continuing education programs.57-58
Homeopathy - An Overview
The Role of Homeopathy in Oncologic Palliative Care
Conclusion
Homeopathy is a widely used treatment approach for different types of pain. As consumers increasingly seek complementary alternatives to conventional analgesics, pharmacy professionals are positioned to guide safe and informed use of homeopathic products by becoming knowledgeable with their principles, manufacturing, regulations, and evidence base to provide safe and effective patient care.